

This article follows on from the previous general article on tooth extraction techniques (Oxford, 2018a), as a specific guide to the extraction of the mandibular canine in dogs. Extraction of the maxillary canine has also been described in detail (Oxford, 2018b). The mandibular canine is a large tooth that is difficult to extract and often leaves a sizeable defect when extracted. Extraction is made more challenging by the shape of the canine tooth, which angles towards the midline, and because the mandible is a very hard bone that does not compress easily. An open extraction is therefore usually the most appropriate technique, as this will allow a more controlled loosening of the tooth. It will also allow suitable closure of the extraction site following extraction.
Mucoperiosteal flap design
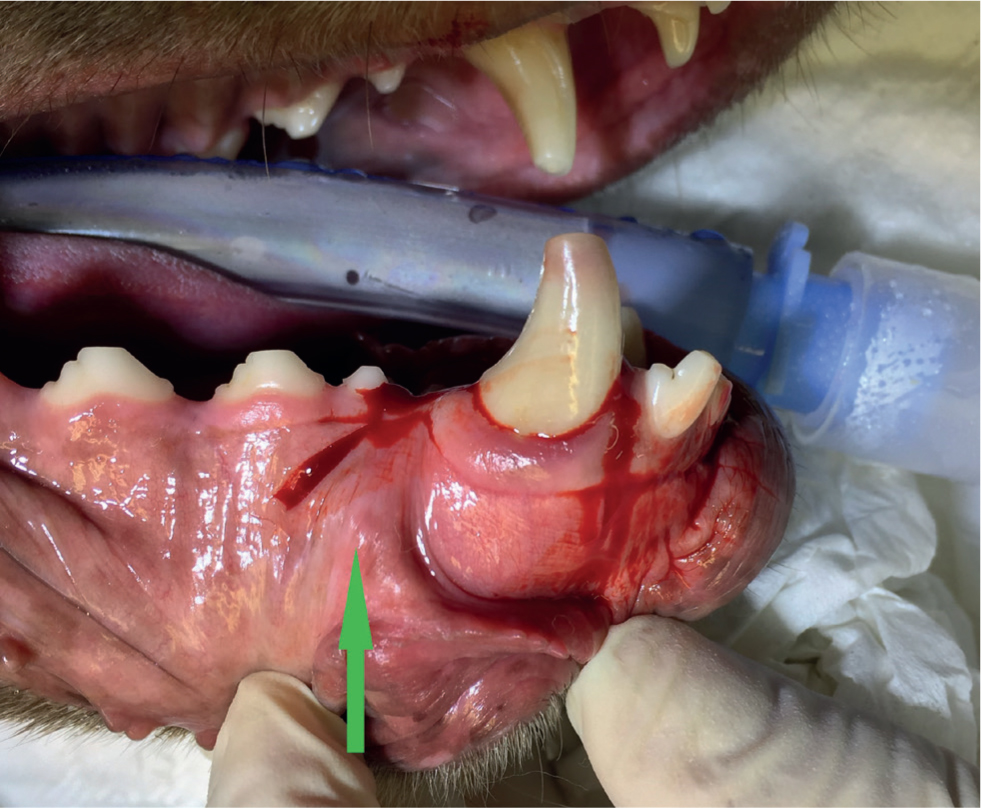
The tooth has a long root, and extensive alveolectomy is often required to facilitate the extraction. A pedicle flap is therefore usually the most appropriate flap to use. Releasing incisions should be made over areas where the bone will still be intact following extraction. A mesial (rostral) releasing incision should be made on the distal (caudal) aspect of the ipsilateral mandibular 3rd incisor. The incision should be extended beyond the mucogingival junction. The incision should then extend around the gingival sulcus and should then cross the alveolar crest across the diastema between the canine tooth and the 1st premolar. The distal (caudal) releasing incision should be made either just mesial (rostral) to the ipsilateral mandibular 1st premolar or in the interproximal space between the 1st and 2nd premolars (Figure 1). The decision here will depend on how closely positioned the mandibular premolars are, but it is important to ensure adequate exposure. The distal releasing incision should then extend obliquely on the caudal edge of the labial frenulum, so that the frenulum is contained within the flap.
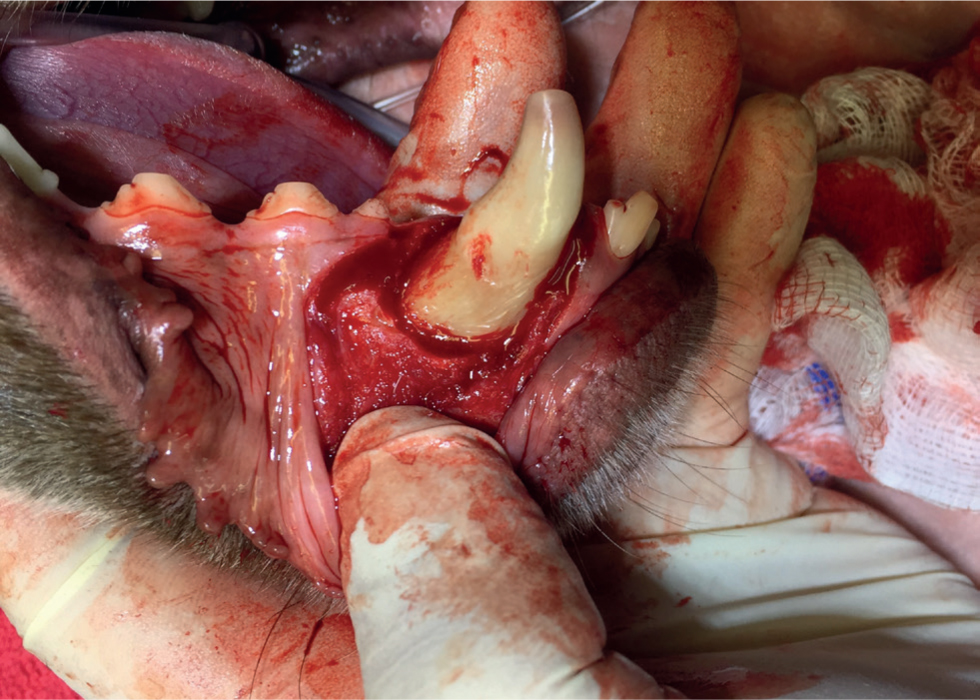
Elevation of the flap using a periosteal elevator is as previously described (Oxford, 2018a). During flap elevation, care must be taken around the middle mental foramen and the neurovascular bundle there. If the periosteum is elevated carefully from the bone then the foramen can be exposed, as the neurovascular bundle is superficial to the periosteum. The middle mental foramen marks the apical extent to which an alveolectomy can be extended (Figure 2).

Alveolectomy
Adequate partial alveolectomy is carried out to facilitate the extraction. Typically, this would be 30–50% of the root length on the buccal aspect of the root. An idea of the tooth root length can be obtained from a dental radiograph, which should be taken before any dental extraction Note that the middle mental foramen marks the apical extent of the possible alveolectomy (Figure 3) (Oxford, 2018a). It is important to remember that, owing to the angulation of the canine tooth, the buccal bone becomes thicker as one progresses apically.
Extraction technique
Mostly, the use of first-class leverage will be required in order to extract the tooth. The elevator is firstly seated firmly between the tooth and the bone on the mesial aspect, then rotational force is applied along the long axis of the tooth (Oxford, 2018a). Additionally, luxation, as previously described (Oxford, 2018a) can be an important technique for this tooth, as excessive elevation force can lead to iatrogenic fracture when extracting this tooth, particularly when elevation force is applied on the lingual aspect where the bone can become thin.
Post extraction
Any periodontal pocket epithelium or inflammatory tissue in the periapical area should be removed along with any calculus. An alveoplasty should be carried out to smooth the alveolar rim. A periosteal releasing incision should be carried out to ensure adequate flap mobility for closure of the extraction site. The mucoperiosteal flap should be closed with simple interrupted sutures, 3 mm apart (Figure 4) (Oxford, 2018a).

Conclusions
Extraction of the mandibular canine tooth in a dog is a challenging surgical procedure. Many surgical complications exist, therefore a good surgical technique is required. A good mucoperiosteal flap and adequate bone removal will facilitate both efficient extraction and closure of the extraction site.
KEY POINTS
- Extraction of the mandibular canine tooth in a dog is a challenging surgical procedure.
- Good surgical technique is important to minimise the risk of complications.
- Efficient extraction and closure of the extraction site are facilitated by a mucoperiosteal flap of sufficient size, and by adequate bone removal.