


When anaesthetising veterinary patients, it is recommended to intubate them with an appropriately sized and type-specific endotracheal tube (ETT), if the species can be intubated. This is especially important when using a volatile inhalant or if the patient requires manual or mechanical ventilation. This ensures there is no environmental pollution, provides personnel safety within the theatre, and delivers the volatile inhalant with 100% oxygen. The 100% oxygen will increase the fraction of inspired oxygen (FiO2) in the patients to prevent hypoxia, leading to hypoxemia. Therefore, increasing the FiO2 will increase the partial pressure of oxygen in the arterial blood (PaO2). With 100% oxygen, patients should have a PaO2 of 500 mmHg (5x FiO2) if a blood gas analysis was performed (Crawford, 2010).
Intubation reduces the risk of desaturation, prevents gas leakage and provides supported ventilation while protecting the airway from regurgitation and aspiration (Nutt et al, 2014). Other indications include emergencies, airway obstruction, deep sedation and patients with airway disease (Auckburally and Flaherty, 2017).
Intubation requires knowledge of the patient's anatomy, the appropriate technique for the species to achieve a patent airway and the need for any additional equipment if there is concern for difficult intubation. Examples of such equipment include an extra laryngoscope blade, a range ETTs and long-tipped swabs. It is also important to understand the correct size and appropriate length of the ETT for the species requiring anaesthesia.
If the ETT is cuffed, the cuff should be inflated to ensure there are no leaks. Lubrication should be used if appropriate, and the patient must be adequately anaesthetised before attempting intubation. Additionally, it is important to plan how the ETT will be secured (Phillips, 2018). Additionally, successful endotracheal intubation relies on correct patient positioning (Bryant, 2009).
Measuring the endotracheal tube
The ETT length is required to be measured in smaller species. This is performed by having the ETT next to the animal's head and ensuring that the ETT is between the canines and the thoracic inlet to prevent bronchial intubation (intubation of one bronchus). The ETT should not be going past the scapula, the point of the shoulder (Phillips, 2018) (Figure 1). If the ETT enters one bronchus, the patient will only have one lung contributing to ventilation; this will increase the risk of hypoxia, leading to severe cyanosis (Bryant, 2009). This can result in a reduction in oxygen saturation (SpO2) and an uneven anaesthetic depth. Once measured, a long ETT should be cut to size, ensuring the adaptor is firmly replaced on the tube. Avoid cutting below the pilot balloon line to reduce the risk of bronchial intubation and decrease mechanical dead space (Gibson, 2024).

Types of endotracheal tubes
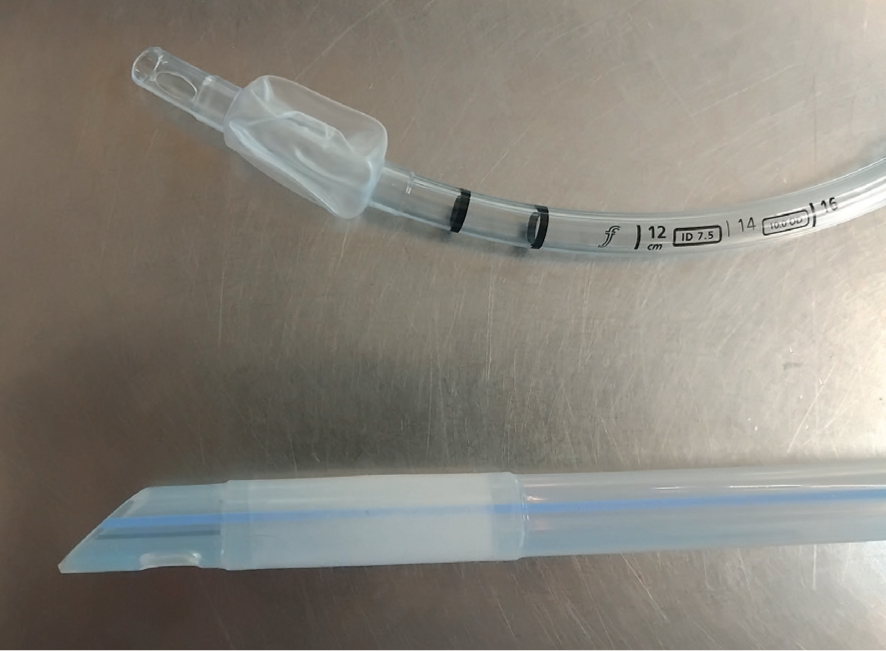
ETTs are manufactured from polyvinyl chloride (PVC), silicone or red rubber. The main types of ETTs are Magill, Cole and red rubber tubes, with the more modern variant being Murphy tubes, which can be cuffed or non-cuffed. An armoured tube, featuring a coil embedded in its wall to prevent kinking, is also available. Armoured tubes are recommended for certain ophthalmic procedures, head and neck surgeries, or cisternal punctures (Hughes, 2016).
A commonly used type of ETT is the Murphy tube. This features a Murphy eye, which is a hole located in the bevel or tip of the ETT, acting as a safety feature. The Murphy eye allows for emergency ventilation if the tube becomes occluded by mucus, blood, debris or contact with the tracheal wall (Bryant, 2009). Murphy tubes are typically made from PVC or silicone, particularly in larger sizes (Auckburally and Flaherty, 2017).
Red rubber tubes, which are rarely seen with a Murphy eye, are generally not ideal because of their drawbacks. Blockages within the tube are not visible, they kink easily (especially when old), and they can irritate the trachea. These factors make red rubber tubes less suitable for use (Hughes, 2016).
Cole tubes, on the other hand, are uncuffed and primarily used in avian patients. Birds have complete tracheal rings, meaning cuffed tubes can cause damage or even tracheal rupture. Cole tubes feature a narrow distal end and a wider proximal end. The distal end, up to the shoulder, is inserted into the trachea through the glottis, forming a seal.
ETT cuffs are available in two types: high-pressure, low-volume and low-pressure, high-volume. High-pressure, low-volume cuffs provide effective airway protection but are more likely to cause injury to the tracheal mucosa. These cuffs are characterised by their smooth appearance when deflated and are often made of silicone. Low-pressure, high-volume cuffs distribute pressure over a wider area, reducing the risk of mucosal trauma. When deflated, these cuffs appear wrinkled and are often made from PVC. However, low-pressure cuffs can allow liquid to pass through the folds created when inflated. To minimise this risk, applying lubricant after inflating the cuff is recommended (Hughes, 2016) (Figures 2, 3).

Difficult intubation
Intubation may be challenging because of a patient's conformity, such as an anatomical abnormality (such as a mass obstructing the airway or a fractured jaw) or a breed-or species-specific difficulty. For example, brachycephalic animals with severe airway obstruction or small mammals with narrow dental arcades may pose unique challenges. Proper positioning of these patients is crucial to securing a successful airway. It is also recommended to pre-oxygenate these patients for at least five minutes to prolong the time before desaturation during intubation.
For difficult intubation cases, it is essential to prepare additional equipment, including:
Having an experienced assistant available to provide support can also be invaluable in such cases (Alleiler, 2022). Figure 4 shows an obscured view in a brachycephalic patient after intubation.

Conclusions
Before exploring techniques for endotracheal intubation in common species, it is crucial to understand the importance of intubation, recognise the common types of tubes available, know how to measure and correctly trim new ETTs in practice, and prepare adequately for potential difficulties during intubation.