


Comerford et al (2006) performed studies on tibial anatomy to determine if there were any identifiable anatomical features which might be correlated with the presence of cruciate ligament disease, finding the anatomy of the femoral intercondylar notch to be the only consistent feature. Ragetly et al (2012) also found that radiographic combination of high tibial plateau angle and femoral anteversion angle are anatomical features that can be used to identify dogs at high risk of cruciate ligament disease. A discrepancy in tibial length has not been identified previously in the veterinary literature as anatomical feature to identify dogs at greater risk of cruciate ligament disease.
It has been reported that changes in the femur:tibia length ratio influence ligament development (Doige et al, 1978; Leipold et al, 1978; Baird et al, 1994; Johnson et al, 1994; Speigel et al, 2003; Kowaleski et al, 2012; Towle and Bruer, 2012). In most cases, the specific cause of long bone deficiency is unknown. Tibial shortening has an identifiable hereditary pattern; the presence of extraskeletal abnormalities in some of these cases, for example cardiac malformation and retained testicles, should suggest that the syndrome may have a familial basis (Poznanski et al, 1971; Doige et al, 1978; Sorge et al, 1995; Bedoya et al, 2015).
Factors that can be implicated in the development of limb length reduction are early compromise of blood supply (for example, amniotic band syndrome), abnormal chondrification, physeal closure. disturbance of mineralisation and endochondral ossification of the growth plate (von Pfeil and DeCamp, 2009), as well as viral infection, bacterial infection, thermal injury and drug toxicity (Boden et al, 1989; Coley, 2013; Kerrigan and Robinson, 2016a).
Achondroplasia is one of the more common bone dysplasias in human and domestic animals and is characterised by a reduction in longitudinal bone growth. This change is most prominent in the shaft with only a slight reduction in length in both the proximal and distal epiphyses (Doige et al, 1978). Short tibia syndrome is caused by a disturbance in both longitudinal bone growth and modelling. In terms of modelling, the process of funnelisation, cylindrisation and remodelling of the tibia appeared abnormal in several studies (Doige et al, 1978; Sorge et al, 1995; Kowaleski et al, 2012; von Pfeil and DeCamp, 2009; Kerrigan and Robinson, 2016a). In some cases, the proximal epiphyses had accommodated the associated distal femur by sloping down in a caudolateral direction. This axial draft of the proximal epiphyses of the tibia developed because tibial condyles articulate more with the femoral trochlea than the femoral condyles.
Although computed tomography may be more useful, X-rays remain the main imaging modality for the diagnosis of short tibia syndrome (Doige et al, 1978; Johnson, 1981; Towle and Bruer, 2004; Breur et al, 2011; Coley, 2013; Kerrigan and Robinson, 2016b). Radiography very widely available, accessible and most affordable method in small animal clinics (Swiderski et al, 2008; Barnes et al, 2015) Magnetic resonance imaging (MRI) and ultrasound scans (US) are adjunct imaging modalities that can help to provide better understanding of the pathological conditions associated with tibial shortening. A number of studies have compared computed tomography and radiography for measuring bone length and alignments and some studies have evaluated the repeatability and reproducibility of the radiographic method (Swiderski et al, 2008; Barnes et al, 2015).
The aims of the present study were:
- To describe the radiological findings of short tibia syndrome and assess its possible association with cranial cruciate ligament degeneration in dogs.
- To evaluate the intra- and inter-radiographic observer correlation for the tibial length measured in this study and determine if the method of radiographic measurement was repeatable, reproducible and reliable.
Materials and methods
Animals
A retrospective study for the calculation of limb length discrepancy, with a particular emphasis on the tibia, was made on entire hind limbs radiographs taken from 84 dogs with long progressive ligamentous degeneration and subsequent rupture of the cranial cruciate ligament and a control group.
The control group was subdivided into two groups: group A onsisted of nine dogs that had a definite traumatic injury to the stifle preceding the rupture of the cranial cruciate ligament, with no histopathological evidence of ligament degeneration, and group B consisted of 22 healthy dogs which had no history, clinical or radiological evidence supporting a diagnosis of cranial cruciate ligament degeneration or rupture, but presented with other orthopaedic conditions that required radiographs of both hind limbs to be performed.
Case selection
Dogs were included in this study if they had entire hind limb radiographs, including the stifle and the tarsal joints, stored in the electronic database of the radiology service at the author's referral hospital.
Radiographs taken from both hind limbs of 115 dogs (84 with degenerative cruciate ligament rupture, nine with traumatic cruciate ligament rupture and 22 without any stifle pathology) were reviewed and analysed for limb length discrepancy, with a special emphasis on the tibia. Radiographic changes and evidence of degenerative joint disease in stifles were recorded. Radiographs were made between October 2001 and December 2021.
Dogs included in the study group and control group A all had known cranial cruciate ligament rupture determined by intraoperative findings at the beginning of each surgical treatment, as well as the presence of cranial drawer movement and tibial compression test on orthopaedic examination. In the study group of dogs, clinical examination performed before radiographic examination showed that one limb appeared shorter than the other. Cruciate ligament degeneration had to be confirmed in the study group of dogs, or unsubstantiated in control group A, on histopathological examination. Criteria for exclusion included the presence of neoplastic bone pathology (such as osteosarcoma), conditions which impede the assessment of limb length discrepancy measures such as fractures and dislocations, skeletal immaturity, or incomplete medical or radiographic records.
Healthy dogs selected for control group B were matched to cases included in the study group of dogs, with respect to age, sex, breed and weight, as these factors are likely to cause significant variation in the results. Dogs presumed to be predisposed to cranial cruciate ligament disease on the basis of radiographic combinations of high tibial plateau angle and femoral anteversion angle, stenotic or narrowed distal femoral intercondylar notch dimensions, patellar luxation and ruptured ligaments which result in stifle joint instability were excluded from control group B. Radiographic measurement of the intercondylar notch size was assessed in this study by measuring the notch base width, measured as the distance between the central margins of the subchondral bone of the medial and lateral condyles.
All radiographical examinations were performed under general anaesthesia. Dogs were premedicated with synthaden (Methadone hydrochloride 0.5–1.0mg/kg intramuscular, Animal Care UK) and Dexdomitor (dexmedetomidine hydrochloride 300mcg/m2 intramuscular, Vetoquinol UK). General anaesthesia was induced with Alfaxan (alfaxalone 0.2–2 mg/kg intravenous, Vetoquinol UK) and maintained with inhaled isoflurane (Merial Animal Health UK).
For reversal of the sedative effect of dexmedetomidine, Se-dastop (atipamezole hydrochloride, 0.04 ml/kg intramuscular, Animal Care UK) at an equal volume to dexdomitor was used. Atipamezole hydrochloride was administered 15–60 minutes after dexmedetomidine hydrochloride administration.
Clinical and orthopaedic examinations were performed in all dogs admitted to this study. The age, sex, breed, weight, degree and duration of lameness before presentation were obtained retrospectively from their records.
Radiographic imaging protocol
All radiographs were taken by digital radiographic machine (Un1002, ultrapeer 200 CR 1001, Fuji Prima 2 CR system, Veterinary X-rays) and evaluated with a Digital Imaging and Communications in Medicine Cloud Pacs scanner.
Radiographic measurements were made using image analysis software (Adobe measurement feature) using a ruler tool.
Radiographs for the evaluation of limb length discrepancy were taken in frontal plane craniocaudal and mediolateral views described by Dismukes et al (2007, 2008), Kim et al (2015) and Aghapour et al (2019).
The frontal plane craniocaudal radiographs were performed in dorsal recumbency. The hind limbs were secured to the table in full extension of the hips, stifles and tarsal joints and the tibia was positioned parallel to the cassette/table using a tape or the 20’’ gooseneck stand, which is made of radiolucent material for positioning over the area of interest in order to avoid artificial distortion of the radiographic images. Both hind limbs were taped to the table at the stifle, and again at the hock joints, to retain them in extension, and to avoid rotation and joint flexion. Both hind limbs were similarly positioned and extended so that the long axis of the femur was parallel to the long axis of the tibia, with the stifles slightly rotated inwards, so that both patellae were pointing up and the caudal aspect of the stifles lay flat on the table. True frontal positioning of the hind limbs was determined by positioning the patella in the center of the trochlear sulcus, both medial and lateral fabellae bisected by their respective femoral cortices; 50% of the lesser trochanter can be seen at the proximal medial femur, the medial edge of the calcaneus aligning near the distal intermediate ridge of the tibia between the cochlea of the tibia. Appropriate positioning was confirmed by fluoroscopy. The mediolateral views were taken in lateral recumbency. The X-ray beam was centered at the mid-diaphysis of the tibia and the tibia was placed parallel to the cassette/table to prevent foreshortening. Appropriate positioning was confirmed with super imposed femoral condyles in view using fluoroscopy. Cotton wool or a radiolucent wedge placed under the hock joint to aid in super imposing the femoral condyles. The tibia was positioned parallel to and in close contact with the table/cassette to prevent fore shortening to allow true size radiograph before measurement were taken.
Clear and well-defined landmarks on the bone itself were used to determine tibial length and total leg length measurement:
- Point A: centre of the medial tibial plateau in the craniocaudal view
- Point B: centre of the distal articular surface of the tibia in the craniocaudal view
- Point C: centre of the proximal articular surface of the tibia in
- Point D: centre of the distal articular surface of the tibia in the mediolateral view.
Calculation of limb length discrepancy was performed using the technique described by Helms and McCarthy (1984), Aiken et al (1985), Glass and Poznanski (1985), Aron et al (1992), Tomlinson et al (2007), Dismukes et al (2007), Sabharwal and Kumar (2008), Olimpo et al (2016), Zilincik et al (2018) and Aghapour et al (2021).
The following measurements were obtained, as they were considered a ‘gold standard’ measurement in the aforementioned studies: Right and left tibial lengths, determined in the craniocaudal view by measuring the distance between the centre of the medial tibial plateau (A) and the centre of the distal tibial articular surface (B) and in the mediolateral view, by measuring the distance between the centre of the proximal articular surface of the tibia (C) and the centre of the distal articular surface of the tibia (D). Total leg length was measured from the centre of the top of the femoral head and the centre of the distal articular surface of the tibia.
Radiological analysis of limb length discrepancy measures
Radiographic measurements that were obtained in the study group population of dogs and the control group of dogs for the left tibial shaft length (LT), right tibial shaft length (RT), right femoral shaft length (RF), left femoral shaft length (LF) and total hind limb length (TLL) were used to calculate femoral shaft length differences (RF–LF), tibial shaft length differences (RT-LT) and hind limbs length discrepancy measures (RHL–LHL).
A comparison was then made between hind limb length discrepancy measurements obtained in the study group and the control group to determine the possible relation between inherent tibial length discrepancy measures and degeneration of the cranial cruciate ligament.
To increase the accuracy, validity and reduce the potential bias of the observer's radiographic measurement of the tibias. Radiographs of each dog were investigated by two recognised specialists in diagnostic imaging and one RCVS recognised orthopaedic specialists to determine if the radiographic measurement protocol of tibias is repeatable, reproducible and accurate. The measurements for each radiographic observer were grouped as first and second round measurements to evaluate the intra-observer variability, and the measurements of all three observers were grouped to evaluate the inter-observer variability. Inter-observer variability was based on a comparison between the three observers to evaluate the reproducibility of the measurement protocol. An average reading was made of all three observers to establish a reference range and specify the quantitative measure and tibial length discrepancy measures. The intra-class correlation coefficient was calculated from the first and second round of measurements taken by each radiographic observer and the inter-class correlation coefficientwas calculated from the repeated measurements made by all three observers.
Inter-class coefficient ranged from 0 (no agreement) to 1 (full agreement) was calculated, and a score > 0.75 was considered high correlation (0.74–0.60 correlation was considered good correlation, 0.4–0.59 correlation was considered fair correlation and a correlation <0.40 was considered poor correlation) (Cicchetti, 1994). Radiographic images were anonymised before measurements were made.
Radiographic assessment of osteoarthritis in the stifle joints
Evidence and severity of the radiographic changes of degenerative joint disease of the stifles, such as osteophytosis, subchondral bone cysts, sclerosis, joint space narrowing and intra-articular joint mouse, were documented.
Assessment of limitation of limb function
The degree and severity of lameness was assessed on clinical and orthopaedic examinations. The duration of lameness before presentation was obtained from the history records.
Correlation between the degree of tibial length discrepancy measures, duration and severity of stifle joints degenerative disease and the duration and severity of lameness was determined using the Pearson correlation matrix.
Assessment of cranial cruciate ligament degeneration
The progress of cranial cruciate ligament disease; cranial cruciate ligament swelling and tears, partial rupture or complete rupture was established at the beginning of each surgery.
Cranial cruciate ligament rupture was determined by intraoperative findings and the presence of cranial drawer movement and tibial compression tests on orthopaedic examination.
Gross pathological, histological and immunohistochemical examinations were carried out on ruptured cranial cruciate ligaments at the beginning of each surgery. Biopsies were collected from the ruptured cranial cruciate ligaments of dogs in the study group and group A of the control group. The samples were fixed in 10% formalin and submitted for examination. Correlation between tibial length discrepancy measures and cranial cruciate ligament degeneration and rupture was determined in an attempt to determine the possible relationship between the inherent tibial length discrepancy measures and cranial cruciate ligament degeneration and eventual rupture.
Statistical analysis
Correlations between the inherent tibial length discrepancy measurements and cranial cruciate ligament degeneration and rupture were determined. Correlation between tibial length discrepancy measures, duration and degree of lameness, and severity and duration of the radiographic changes of degeneration in the stifles, was determined in the study and control groups using the Pearson correlation matrix. Winks statistical data analysis software was used for statistical analysis of the Pearson coefficient.
Pearson correlation coefficient (r) is the most common way of measuring a linear correlation. Its value ranges between -1 and 1, -1 indicating a strong negative correlation between the variables, 0 indicating no correlation and 1-indicating a strong positive relationship between the variables.
Two sample students' t-test with separate variances were used to measure the correlation between the two variables and statistical significance was set at P<0.05. A comparison was then made between the results in the study group and the control group, so the clinical relevance of the findings could be interpreted.
Results
Clinical analysis
A total of 115 client-owned dogs treated at the author's referral hospital were included in this study. Their weight ranged from 9–85 kg (mean 35 kg). Their age ranged from 1.9–8.6 years (mean 5.2 years). There were two intact females, 70 neutered females, two intact male and 41 neutered males. Breeds included; Labrador Retriever (n=34), Golden Retriever (n=20), Rottweiler (n=11), Newfoundland (n=8), English bull mastiff (n=6), Boxer (n=4) Doberman Pinscher (n=4), Staffordshire Terrier (n=4), Saint Bernard (n=4), mixed breeds (n=3) and one individual from 17 other breeds.
Dogs included in the study group and group A all had stifle instability and cranial cruciate ligament rupture confirmed using cranial drawer movement and tibial compression test on orthopaedic examination. On clinical examination, when both hind limbs were extended caudally before the radiographic examination, one limb appeared shorter than the other, and the distance between the hock and stifle was obviously reduced in the shorter limb.
Radiographic analysis of limb length discrepancy measurements
Radiographs were made with an intensity ranging from 2.6–3.8 milliampere per second and penetrability ranging from 48–52 kilovoltage peak. Radiographs of the hind limbs in 84 dogs in the study group, that had no trauma before the rupture of the cranial cruciate ligament, appeared to have one tibia shorter than the other. The normal cylindrical configuration was altered to the extent that in some cases, the bone appeared rectangular, with the proximal epiphysis sloping down in a caudolateral direction. Examples can be seen in Figure 1 and Figure 2.


Notable discrepancies were found in tibial length that significantly departed from null of symmetry (P=0.0001). In the 84 included in the study group, 52 (61%) had tibial asymmetry of 3mm or more, 18 dogs (21%) had a difference of 5mm or more and 14 (16%) had tibial asymmetry of 7 mm or more. Average tibial discrepancy measurement of all three radiological observers was 6 mm (Table 1)
Table 1. Inter- and intra-observer average tibial discrepancy measurement in 84 dogs included in the study group
| Tibial asymmetry measurement | Number of dogs | Inter-observer average of tibial discrepancy measurement reading | Intra-observer average of tibial discrepancy measurement readings | ||
|---|---|---|---|---|---|
| Observer 1 | Observer 2 | Observer 3 | |||
| 3mm or more | 52 (62%) | 4mm | 3mm | 4mm | 5mm |
| 5mm or more | 18 (21%) | 6mm | 5mm | 6mm | 7mm |
| 7mm or more | 14 (17%) | 8mm | 7mm | 8mm | 9mm |
The study of the discrepancy measures of the tibias showed that observer 1 had a lower radiographic discrepancy measure than observer 2 and 3. In general, there was good to high correlation between all three observers.
The inter-observer variability was based on the measurements between the three observers to evaluate the reproducibility of the measurement procedure. The inter-observer inter-class correlation coefficient) was greater than 0.75 for 67% of the measurements, indicating high correlation, and the remaining 33% of the measurements were between 0.6 and 0.74, indicating good correlation. The average inter-observer inter-class correlation coefficient was > 0.75 for tibial measurement, indicating high reproducibility.
The intra-observer intra-class correlation coefficient for the tibial measurements of the first observer were >0.75 for 61% of the measurements, indicating high correlation, and between 0.6 and 0.74 for 39% of the measurements, indicating good correlation. For the second observer, 89% of the measurements were greater than 0.75, indicating high correlation, and just 11% of the measurements were between 0.6 and 0.74, indicating good correlation. For the third observer, 77% of the measurements were greater than 0.75, indicating high correlation and 23% of the measurements were between 0.6 and 0.74, indicating good correlation. The average intra-class correlation coefficient was >0.75 for tibial measurements, indicating high repeatability.
These results show that tibial measurements were repeatable and reproducible and between the three observers. Therefore, the selected tibial radiographic measurement protocol described in this study has good to high correlation, and was dependable and reliable in measuring tibial length discrepancy.
In the study group, the average left tibial length was 12.7cm; the average right tibial length was 13.3 cm and the tibial difference was 6mm. One fifth of dogs with a short tibia also had a measurement discrepancy between the left and right femur; the average total limb length discrepancy was 8mm.
No significant inherent tibial length discrepancy measurements were found in control group A or B; in group A, 89% (8/9) of dogs had no tibial asymmetry measurement and the average left tibial shaft length and right tibial shaft length was 13.8cm. Only one dog in this group (11%) had a tibial length asymmetry of 2mm; the left tibial length was 12.20 cm and the right tibial length was 12.40 cm and total limb length discrepancy was 0.2 mm. The average tibial length discrepancy measure in control group A was 0.2mm.
In control group B, 18 dogs (82%) had no tibial or femoral asymmetry, average left and right tibial length in the 18 dogs were 13.2cm. Four dogs (18%) had an average tibial length asymmetry of 1mm, the average right tibial length in the four dogs was 12.4 cm and the average left tibial length in the 4 dogs was 12.5cm. The average total limb length discrepancy in the four dogs was 2mm.
The average tibial length discrepancy measure in control group B was 0.2mm. The difference between average tibial length discrepancy measurements in the study group of dogs and control group of dogs was 5.8mm. There was a correlation between tibial length discrepancy measures, radiographic changes of degenerative joint disease of the stifles, and the degree and duration of limb function limitation and cranial cruciate ligament degeneration and rupture in the study group.
Evidence and severity of degeneration in the stifle joints in the study group
Progressive radiographic evidence of degeneration of the stifles was seen in the study group:
- Joint effusion and a radiodense infrapatellar fat pad (gray cloud) was seen at the beginning of cruciate ligament disease and preceded the complex progressive degenerative joint disease
- Joint space reduction of the medial aspect of the stifle joints progressed from 0.7 mm to a non-recognisable medial stifle joint compartment
- Osteophyte and sclerotic lesions measurement ranged from less than 1 mm to more than 7 mm
- Intra-articular joint mouse lesions and subchondral bone cysts were only seen in the late stages of severe degenerative stifle joint disease.
Degree and duration of lameness:
Varying degrees of limb function limitation were seen:
- Mild limb function limitation: the affected limb was carried with the stifle slightly flexed
- Moderate limb function limitation: the dog used the affected limb when walking, but at rest stood with toe just touching the ground
- Severe limb function limitation: lameness was often insidious in onset and suddenly became worse and progressed to non-weight bearing lameness.
The duration of lameness in the 84 dogs in the study group varied from 5–36 months.
The greater the degree of tibial length discrepancy, the more apparent the limb functional limitation and the more severe radiographic changes of degenerative stifle joint disease.
Tibial length discrepancy of 3–5 mm was found to be associated with mild limitation in limb function and mild radiographic changes of degenerative stifle joint disease (Table 2). Tibial length discrepancy of 5–7 mm was found to be associated with moderate limitation of limb function and moderate radiographic changes of degenerative stifle joint disease. Tibial length discrepancy of more than 7mm was found to be associated with severe limb function limitations and severe radiographic changes of degenerative stifle joint disease.
Table 2. Correlation between tibial length discrepancy measures and degree of lameness
| Tibial length discrepancy measures | ||
|---|---|---|
| 3mm-5mm | 5mm–7mm | More than 7 mm |
| Mild degree of lameness. | Moderate degree of lameness | Severe degree of lameness |
Histology and immunohistochemistry of the ruptured cranial cruciate ligament
Gross pathological appearance of the ruptured cranial cruciate ligament was classified as ‘normal’ or ’abnormal’ (thinned or hypertrophied).
In nine dogs in the control group, the gross appearance of the cranial cruciate ligament was found to be ‘normal’ but completely ruptured, with no histological evidence of degenerative disease (Figure 3). The gross pathological appearance was found to be ‘abnormal’ in the 84 dogs in the study group (thinned in 31 and hypertrophied in 53).

Four types of degenerations were noted on the histological examinations of the ruptured cranial cruciate ligament in this group (Figure 4):
- Mucoid degeneration in seven dogs
- Hyaline degeneration in 12 dogs
- Liquefaction in 36 dogs
- Calcification in 29 dogs.

Short tibia syndrome was consistently found to be associated with stifle joint instability, cruciate ligament disease and progressive osteoarthritis.
Cranial cruciate ligament degeneration and rupture consistently presented first in the limb that exhibited radiographic evidence of short tibia syndrome. When cruciate ligament rupture developed in the other limb, dogs typically presented at a later time.
Control group A
All nine dogs in group A presented with acute non-weight-bearing lameness. Radiographic examinations performed soon after the injury of the stifles confirmed joint effusion, seen as a reduction or obliteration of the fat pad and caudal displacement of the facial planes, no other orthopaedic condition or neoplasia could be detected on radiological examination. Osteophytes as a signs of secondary osteoarthritis were not detected in any of the radiographs.
Control group B
All 22 dogs included in group B had no history, clinical or radiological evidence supporting a diagnosis of cranial cruciate ligament degeneration or rupture.
Statistical analysis
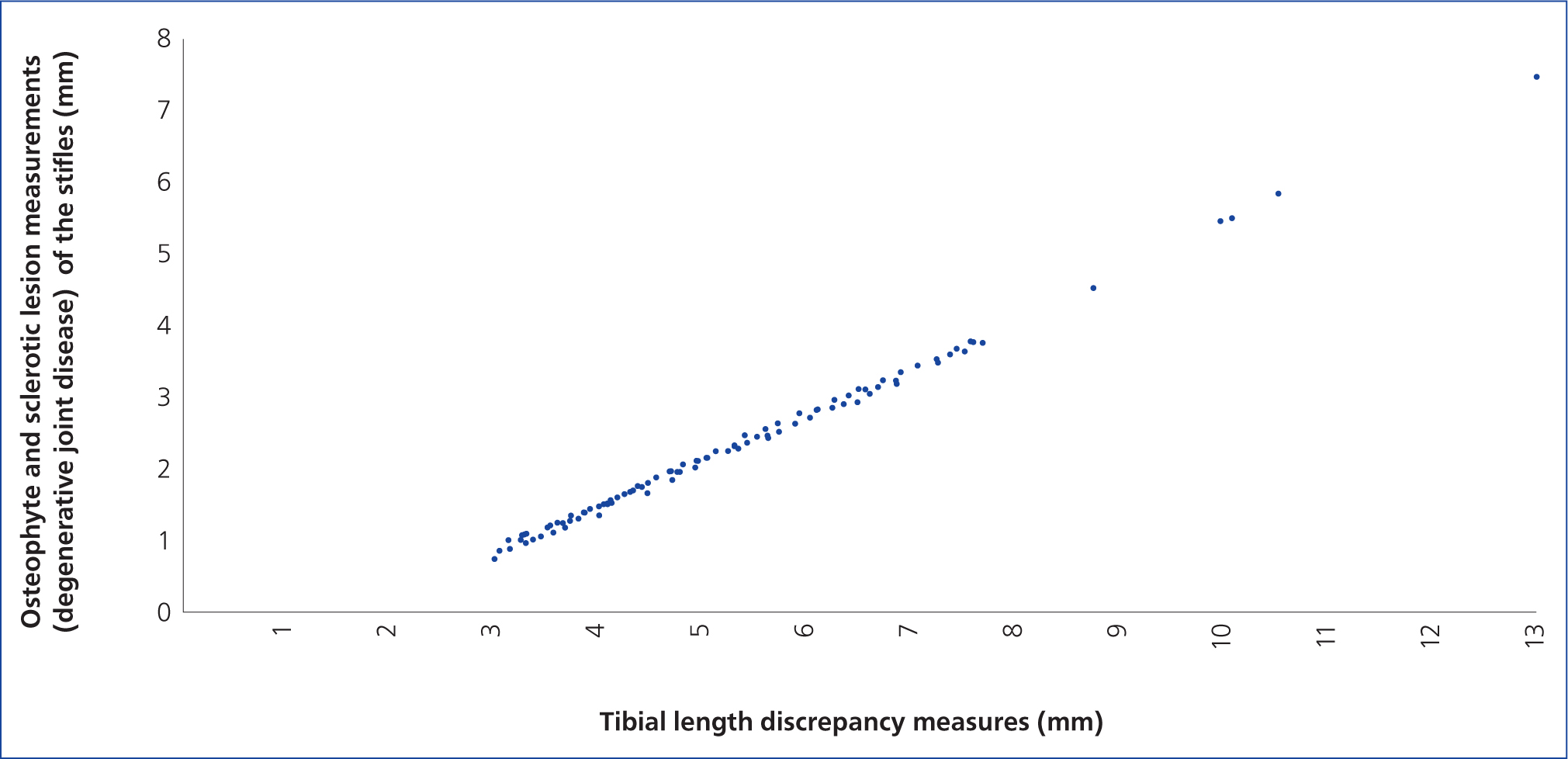
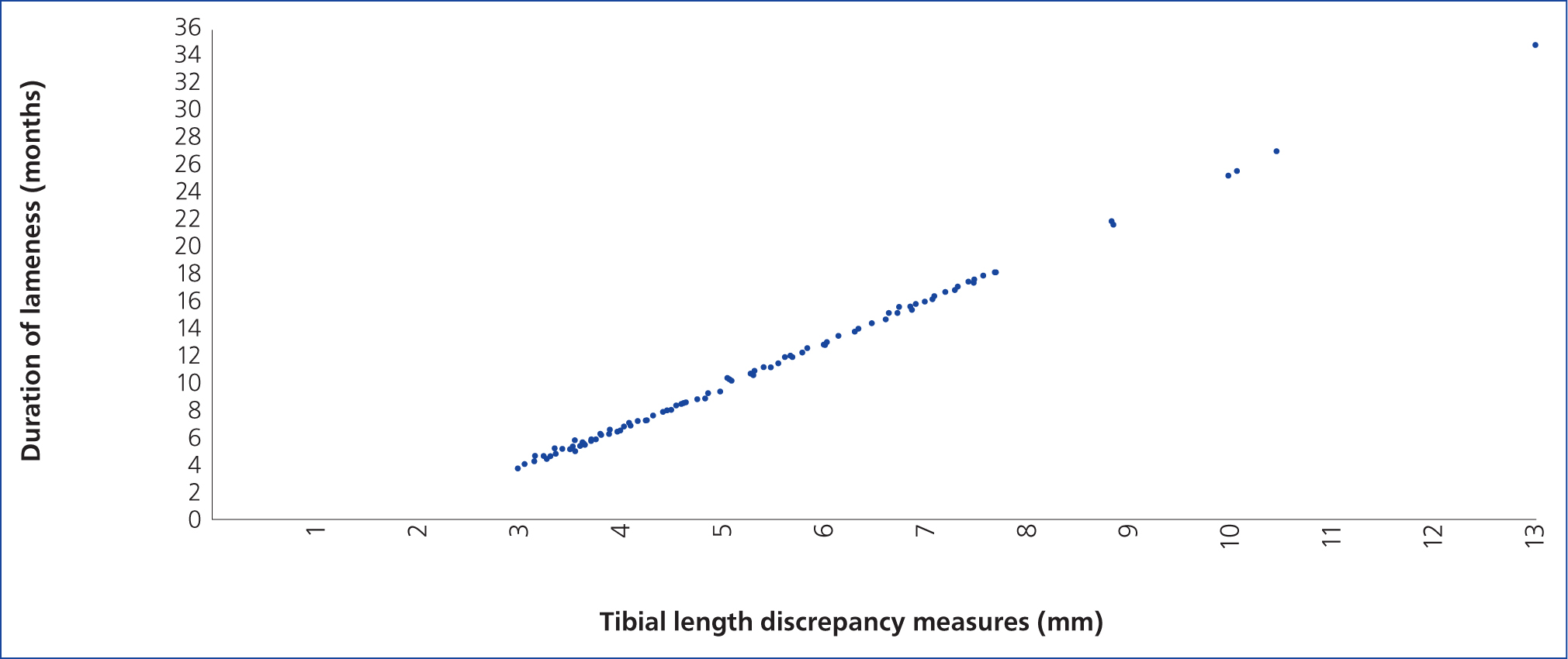
In the study group, tibial length discrepancy measurements were positively and highly correlated to cranial cruciate ligament degeneration, stifle instability and rupture. The degree of tibial length discrepancy measures was found to be positively and highly correlated to the severity of the radiographic changes of degeneration in the stifle joints (correlation of almost +1 on Pearson correlation coefficient test; Figure 5). The degree of tibial length discrepancy measures was found to be positively correlated (R= 0.894 on Pearson correlation coefficient test) to the duration and degree of lameness (Figure 6; Table 2).
In the control group, there was no correlation between tibial length discrepancy measures and cranial cruciate ligament disease and stifle joint degeneration and limb lameness (Pearson correlation coefficient; R=-0.5). It could not be judged whether the change in one variable was directly or inversely proportional to the other variables. Stifle joint degeneration was not detected. Limb lameness in group A of the control group was directly related to traumatic cruciate ligament rupture, with no evidence of cranial cruciate ligament degeneration.
The data collected for tibial length discrepancy of 31 dogs in the control group were insignificant and thus difficult to plot. The scatterplots were far away from the line and it was practically impossible to draw a line.
These observations support the hypothesis that limb length discrepancy measures may contribute to cranial cruciate ligament degeneration and subsequent rupture.
Clinical significance
Short tibia syndrome may be a significant factor predisposing dogs to cranial cruciate ligament degeneration and its associated findings (such as rupture, degenerative disease of the stifle joint and grade of lameness). Dogs with short tibia syndrome may also require surgical correction to treat cruciate ligament disease.
Discussion
Tibial shortening has an identifiable hereditary pattern; the presence of extra-skeletal abnormalities in some of these cases, such as cardiac malformation and retained testicles, suggest that the syndrome may have a familial basis (Pozananski et al, 1971; Doige et al, 1978; Sorge et al, 1995; Bedoya et al, 2015).
Some factors that can be implicated in the development of limb length reduction are early compromise of blood supply, premature physeal closure, disturbance of mineralisation, and endochondral ossification of the growth plate (von Pfeil and DeCamp, 2009), viral infection, bacterial infection and drug toxicity (Boden et al, 1989; Johnson et al, 1994; Speigel et al, 2003; Coley, 2013; Kerrigan and Robinson, 2016b).
Short tibia syndrome, and changes in the femur/tibia ratio, have a significant effect on stifle joint biomechanics, influencing several pathological conditions in the stifle joints, and lead to posture deformity, gait asymmetry and abnormal shape and deformity of the tibia (Doige et al, 1978; Johnson et al, 1994; Baird et al, 1994; Spiegel et al, 2003; Leipold et al, 2010; Towle and Breur, 2012; Kowaleski et al, 2012).
In some cases, the proximal epiphyses of the tibia had accommodated the associated distal femur by sloping down in a caudolateral direction. This change in the proximal epiphyses of the tibia developed because tibial condyles articulate more with the femoral trochlea than the femoral condyles (Doige et al, 1978).
The relationship between short tibia syndrome and the progressive, and irreversible, degenerative changes that gradually develop within the cruciate ligament, has been explained in human literature; short tibia syndrome, which causes limb length discrepancy, leads to a significant increase in ground reaction forces on the shorter leg during walking, increasing mechanical stress. Asymmetrical leg lengths seen in short tibia syndrome also result in pelvic tilt or torsion, which increases the magnitude of internal joint load, as well as placing unequal stresses on the stifle, hip, sacro-iliac and lumbar spinal joints. This unnatural increase of the biomechanical forces, and loading stress in the stifle, has direct, grave consequences for ligament development and stability in the stifle, leading to the development of degenerative disorders in the stifle, including progressive and irreversible cranial cruciate ligament degeneration, eventually leading to fatigue and rupture, stifle joint instability, osteoarthritis and pain (Caw and Bates, 1991; Beard et al, 2008; William et al, 2010; Bradley and Castellano, 2011; Klapour et al, 2012; Noll, 2012; Kjowski et al, 2014; Kwee et al, 2015; Murray and Azari, 2015; Khalifa, 2017, Hanna, 2020).
Degenerative joint disease is initiated by the repetitive and continuous unnatural stress of the biomechanical forces, and loading stress in the stifle. While this is not sufficient to cause immediate cranial cruciate ligament rupture, it initiates the complex progressive syndrome of degenerative joint disease and gradual degeneration of the cranial cruciate ligament, starting with a swelling and tear and ending in complete rupture of the ligament. It has been proposed that short tibia syndrome, and the cumulative traumatic injury to the stifle, causes changes in contact surface of the articulating bones and muscle atrophy, directly leading to inflammation of the entire stifle joint component giving rise to degenerative joint disease and instability (Klapour et al, 2012; Noll, 2012; Kjowski et al, 2014; Kwee et al, 2015; Murray and Azari, 2015; Khalifa, 2017).
The biomechanical exposure of the stifle joint upregulates the release of inflammatory mediators, proliferation of inflammatory cells and degenerative enzymes. Intra-articular inflammation induces degeneration of all joint components including cartilage, joint capsule, bone and bone marrow and ligaments. particularly ligaments, which connect with the articulating bones such as the cruciate ligament and meniscotibial ligaments, fixing the fibrocartilaginous menisci to the tibial bone. Abnormal biomechanics and biology definitely potentiate and exacerbate one another (Kwee et al, 2015).
Early cruciate ligament disease often presents with little or no radiographic evidence of degenerative joint disease. The severity of the radiographic changes of degenerative stifle joint disease correlate with the severity and duration of lameness, the progressive degeneration of the cranial cruciate ligament that start with a swelling and tear and end in complete rupture and stifle instability (John et al, 1986; Cook et al, 2010; Vedrine et al, 2013; Kjowski et al, 2014; Aaertsens et al, 2015; Schulze-Tanzil et al, 2019).
Comerford et al (2006) studied tibial anatomy to determine if there were any identifiable anatomical features which correlate with the presence of cranial cruciate ligament disease. They found the anatomy of the distal femoral intercondylar notch dimension to be the only consistent feature and concluded that impingement by the narrowed intercondylar notch dimension on the cranial cruciate ligament resulted in increased collagen remodelling and increased deposition of sulphated glycosaminoglycans, causing reduced structural integrity of the ligament. Altered cranial cruciate ligament composition predisposes the ligament to increased laxity, leading to its degeneration and stifle joint osteoarthritis. This may have an implication for the pathogenesis of the cranial cruciate ligament rupture.
Many methods have been proposed for measuring the distal femoral intercondylar notch size, but these correlate with intraoperative measurements or require computed tomography scanning, which is not readily available in small animal clinics. Notch measurement using radiography, that match intraoperative arthroscopic measurements to identify narrow intercondylar notches, was described by Ravi Vaswani et al (2019); notch base width was measured as the distance between the central margins of the sub-chondral bone of the medial and lateral femoral condyles using a ruler tool.
Ragetly et al (2012) also identified dogs at risk of cruciate ligament disease and found that dogs with high score of radiographic combination of tibial plateau angle and femoral anteversion angle (>1.5) are predisposed to cranial cruciate ligament disease, compared with dogs with a score <1.5 (Ragetly et al, 2012).
To reduce the potential differences of tibial measurements, radiographs were viewed by three specialist observers and average reading of all three observers was taken. It has been reported that radiographs may not be accurate because of difficulties in positioning the tibia (Yasakuwa et al, 2016). Although computed tomography is considered less susceptible to potential artefacts and rotational deformities, there are recognised differences in many parameters in all imaging tools including and there is no significant difference between imaging methods (Dudley et al, 2006). However, in the present study, 67% of the inter-observer coefficients had high correlation and the remaining 33% had good correlation. Intra-observer coefficients for tibial measurements of the first radiographic observer were 61% high correlation and 39% good correlation; for the second radiographic observer, 89% high correlation and 11% good correlation, and for the third observer, 77% high correlation and 33% good correlation was recorded. The results show that the radiographic method used in this study for tibial measurement is repeatable and reproducible by three radiographic observers and the selected radiographic protocol has good to high intra– and inter-observer correlation.
Limitations
The group of dogs selected for the study group all had two confirmed clinical conditions: all had hind limb length discrepancy on clinical examination and stifle instability. Clinical examination performed before radiographic examination showed that one limb was shorter than the other, and stifle instability was confirmed with cranial drawer movement and a tibial compression test on orthopaedic examination. The inclusion of dogs that had significant progressive lameness and stifle instability on orthopaedic examination, but did not have limb length discrepancy on clinical examination, would have assessed the relationship between tibial length discrepancy and degeneration of the cranial cruciate ligament in all dogs, not just those with limb length discrepancy on clinical examination. Future studies are warranted to help to identify and elucidate this specific deformity of the canine tibia.
Conclusions
Treatment strategies should address abnormal biomechanics and biology with the overall goal of improving limb function, reduce pain, and slow disease progression. Dogs with cranial cruciate ligament disease and short tibia syndrome are combatting biomechanical and biological factors that induce and perpetuate degenerative joint disease and exert clinical signs of pain, lameness and limb dysfunction. The combination of hereditary, developmental, biomechanical and biological factors involved in cranial cruciate ligament disease in dogs could be considered a component of a stifle dysplasia complex.