


Conditions affecting the hip are a frequent cause of hindlimb lameness, particularly in the juvenile dog, and include hip dysplasia and Legg-Calvé-Perthes disease (Scott, 1999). In the adult dog, osteoarthritis of the hip (often secondary to hip dysplasia) is common and should be considered in any dog suffering from hip pain, alongside soft tissue injuries in sporting dogs. This article is part of a series and discusses the rehabilitation of the above conditions that affect the hip.
Before referral for rehabilitation, it is important that the animal has undergone a detailed assessment including history taking, physical examination and further investigation if warranted, in order to achieve a diagnosis from the veterinary surgeon. Discussion between the veterinary surgeon and owner will determine whether surgery is necessary (for example, in the case of some cases of hip dysplasia and for dogs suffering from Legg-Calvé-Perthes disease). Whether rehabilitation protocol will be used to assist with recovery from surgery, or whether rehabilitation techniques will be used as part of a conservative management strategy, such as for non-surgical cases of hip dysplasia, or for treatment of a soft tissue injury, should also be discussed.
Soft tissue injuries affecting the hip
Aetiology
According to epidemiological studies, soft tissues injuries account for less than 5% of musculoskeletal disorders, although the true figure may be much higher than this as they are often self-limiting and are not presented to a veterinary surgeon (Ragetly et al, 2009). In the author's experience, the most common soft tissue injury surrounding the hip is an iliopsoas muscle strain. The iliopsoas is an important stabiliser of the hip and vertebral column, and injuries can be acute or chronic in nature. Such injuries are most common among sporting dogs - particularly those involved in agility-based sport, and likely occur as a result of repetitive stress (Cullen et al, 2017). Excessive stretch of the muscle while engaged in eccentric contraction results in the fibres of the muscle becoming disrupted, most often at the tendon of insertion (Cabon and Bolliger, 2013). Animals present with a decrease in hip extension and so a shortened caudal stride on gait assessment, and are painful during hip extension and internal rotation of the hip on examination (Ragetly et al, 2009). Diagnosis is achieved by observing the animal for signs of pain on palpation at the tendon of insertion, or by imaging via ultrasound (Cullen et al, 2017).
Goals
The goal of treating an iliopsoas injury is complete return to function for the dog, and for the prevention of both long-term issues relating to lack of ‘normal’ limb use and re-injury.
Skeletal muscle injuries undergo three phases of healing: the inflammatory phase, the proliferation phase and the remodelling phase.
Treatment
For the first 72 hours following injury (the inflammatory phase), treatment should be focused on rest, cryotherapy and pain relief, generally in the form of non-steroidal anti-inflammatories (NSAIDs) for 5–10 days (Cabon and Bolliger, 2013). Immobilisation during rest minimises haemorrhage and allows for the formation of granulation tissue. Results from human studies suggest that patients should be rested completely before beginning physical therapy for rehabilitation, for 5–10 days according to the severity of the injury (Cabon and Bolliger, 2013).
Because of the deep location of the iliopsoas muscle, the benefits of cryotherapy (including reduction in oedema, haemorrhage, and pain, and penetration 1–4cm into the tissues) may be limited in larger patients, but application of a cold pack to the groin area for 5-15 minutes three times daily should still be attempted for the first 72 hours following injury, to address inflammation in the local but more superficial soft tissues (Cabon and Bolliger, 2013).

During the proliferation phase, the organisation of the deposition of fibrous tissue is improved if load bearing is initiated and tension is applied to the muscle (Cabon and Bolliger, 2013). It is at this stage that rehabilitation therapies would normally be initiated. Manual therapy, which would benefit the animal recovering from iliopsoas injury, includes passive range of motion exercises, stretches and massage (Table 1).
Table 1. Manual therapies for iliopsoas injury
| Recommended exercise and description | Repetitions and frequency | Benefits |
|---|---|---|
| Passive range of motion:With the patient in lateral recumbency and the limb supported by the therapist, the therapist moves the hip joint slowly through flexion and extension until natural resistance is met | 10 repetitions, three times daily | Enhanced vascular and lymphatic circulation which assists healingLimits fibrosis and adhesion formation |
| Massage (Figure 1):A gentle compress and release technique is applied to the affected area | 10 minutes, applied to the iliopsoas area, three times daily | Breaks the cycle of muscle spasm which leads to shortening of tissueReduces pain caused as a result of muscle spasmImproves circulation |
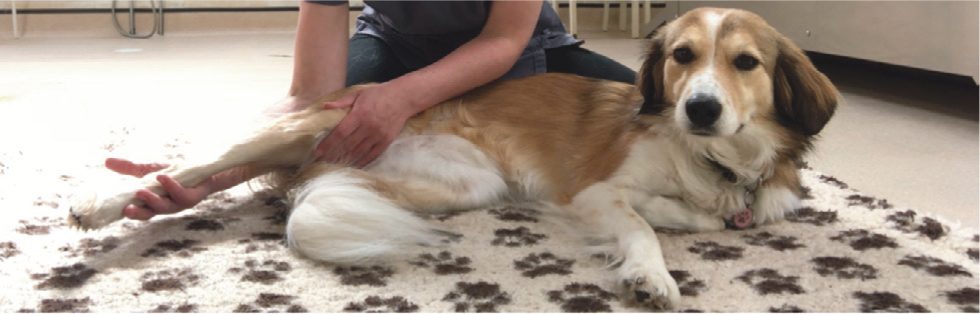
| Stretching (Figure 2):With the patient in lateral recumbency and the limb supported from underneath, the therapist applies gentle pressure mid-femur to extend the hip and hold it in position for 30 seconds | Hold for 30 seconds for three repetitions, three times daily | Assists in the organisation of the alignment of fibrous scar tissuePrevents shortening of muscle tissue through spasm |
Towards the end of the proliferation stage (anything from 5-10 days which can be determined by resolution of any swelling and heat in the muscle), and the beginning of the remodelling phase, exercises to enhance core and hindlimb muscle strength and coordination are initiated. The chances of a favourable outcome following rehabilitation are high, with the majority of dogs in one study achieving a complete recovery following early intervention with physical therapy (Cabon and Bolliger, 2013). There is, as with any muscular injury, risk of reoccurrence, particularly if the injury is not fully healed before recommencing high impact activity (Nielsen and Pluhar, 2005).
Conservatively managed hip dysplasia and osteoarthritis of the hip
Goals
The goals for dogs suffering from hip dysplasia, which is to be managed conservatively, and from osteoarthritis of the hip (which in most cases is secondary to the dysplasia) are the same:
- To reduce pain
- Improve range of motion of the hip joint
- Primarily promote hip extension
- Strengthen the limb
- Improve function.
The hope is that by managing the condition in this way, the progression of arthritis is minimised, and discomfort from compensations is also minimised. The rehabilitation therapist also plays a role in assisting the owner with weight management for the patient, and for exercise and environmental modification to ensure acute-on-chronic flare-ups, as a result of slips/trips in the home and over-exercise, are minimised.
Pain management
Non-pharmacological options for assisting with pain management that can be provided as part of rehabilitation therapy include acupuncture, electrotherapy, thermotherapy and massage (Dycus et al, 2017).
Application of cold in the form of ice packing the affected joint for 5-15 minutes is useful for patients undergoing an acute flare up, as it has been shown to reduce post-traumatic inflammation within the joint. Whereas, for chronically affected animals, application of a heat pack to the affected area (Figure 3) may result in reduced joint stiffness and improved joint function (Oosterveld and Rasker, 1994). The real benefits of heat application are likely to be to the soft tissues, as application of heat improves circulation (Oosterveld and Rasker, 1994) and may help relieve secondary spasm and tension in the muscles surrounding the affected joints, and in the muscles of the back, which are often responsible for secondary pain. Application of heat improves tissue elasticity and is an excellent precursor to massage or stretching (Dycus et al, 2017).

Soft tissue massage techniques including myofascial release are commonly used as a treatment technique to address muscle tension and spasm, often arising as a result of compensations through off-loading body weight from a painful area (the hind quarters) on to a non-painful one (the forequarters), resulting in over-loading. One of the theories behind the pain-relieving benefits of massage is the provision of improved pathways for oxygenation of muscle tissue (Danneskiold-Samsoe, 1999). Oxygen is stored in the muscle as myoglobin, and studies have demonstrated a marked improvement in patient muscle tension and pain levels following increased plasma concentrations of myoglobin after application of massage (Danneskiold-Samsoe et al, 1986). As a large number of patients with orthopaedic disease suffer from secondary soft tissue pain, this treatment modality has a significant place in the management of dogs with hip dysplasia/osteoarthritis.
The potential benefits of acupuncture and electrotherapy, including pulsed magnetic therapy and photobiomodulation to assist with pain management, have been discussed in previous articles in this series, and should be considered as part of a rehabilitation programme for the management of hip pain.
Improving range of motion and strengthening
A combination of passive and active range of motion exercises and stretching techniques works best to improve joint range of motion, which in turn assists with the management of joint pain.
Dysplastic hips are most likely to suffer from a reduction in joint extension (Dycus et al, 2017). So, when initiating passive range of motion techniques, extension of the hip joint may be extremely limited depending on the severity of the condition, and perhaps also on the age of the dog. As one study demonstrated, Labradors affected by hip dysplasia had a reduction of available hip extension of around 1° per year (Greene et al, 2013). A severe reduction in hip extension is likely to affect the dog's functional ability to climb stairs, jump up onto furniture, and in and out of the car, so aiming to maintain or improve hip extension is important for the performance of everyday activities. Passive range of motion exercises are described above. Application of gentle pressure at the end of range, and holding for at least a few seconds (10 is optimum), is defined as stretching (Dycus et al, 2017) and is most effective when the tissue is warm.
Table 2 describes active range of motion exercises which promote hip extension. These exercises can be performed by the therapist during the session, or in some cases, by the owner as part of a home programme. Many active range of motion exercises also function as strengthening exercises, which have been shown to have a positive impact on human osteoarthritis patients. This is as a result of increased protection for the joints afforded by strengthening the periarticular musculature and, because muscle tissue also serves as a shock absorber reducing impact on painful, arthritic joints (Millis and Levine, 1997).
Table 2. Active range of motion exercises for increasing hip extension
| Recommended exercise and description | Repetitions and frequency | Benefits |
|---|---|---|
| Slow, controlled leash walking | Begin with 15-20 minutes, two to three times daily depending on the dog's capability, adding 5 minutes onto each walk per week if they are progressing well (Dycus et al, 2017) |
|
| ‘Dancing dog’ exercise (Figure 4): Supporting the forelimbs of the dog and walking either forwards or backwards, ensuring the hips do not become over extended. Please note, this exercise is not appropriate for all dogs | Start with a few seconds of standing still, then progress by walking the patient a few steps forwards initially, the backwards as hip extension improves and is more comfortable.Repeat for three sets, three times daily |
|
| Aquatic therapy:Use of the underwater treadmill | Hydrotherapy is most often used on a weekly or twice weekly basis, where the therapist builds up time spent walking during sets, and walking speed gradually |
|
| Sit-to-stand exercises:The dog is asked to sit and therapist/owner is positioned behind the dog to align the stifles medially, if rotated laterally. The dog is then called to stand | Begin with three repetitions and increase gradually.Repeat three times daily In dogs who struggle, this exercise can be performed by asking the patient to sit on the therapist's knee or a block to reduce the challenge |
|
Proprioception and balance
As well as losing muscle strength and range of motion, proprioception may also be reduced in animals suffering from osteoarthritis. It is therefore advantageous to include proprioceptive enhancing balance exercises to a rehabilitation treatment programme (Dycus et al, 2017). Examples of balance exercises which may benefit such patients are:
- Rhythmic stabilisations. These are gentle weight shifting exercises, whereby the therapist applies gentle pressure to shift the patient's weight in a cranio-caudal or medio-lateral direction. These can be performed on a flat surface, or on a ramp to progress the exercise
- Three-legged stands, where the therapist lifts each limb in sequence off the ground, initially by a few centimetres for no more than a few seconds, so that the patient is balancing on three legs
- Use of wobble cushions (Figure 5), where the dog's fore or hind limbs are placed on cushions that create instability and challenge the animal to balance


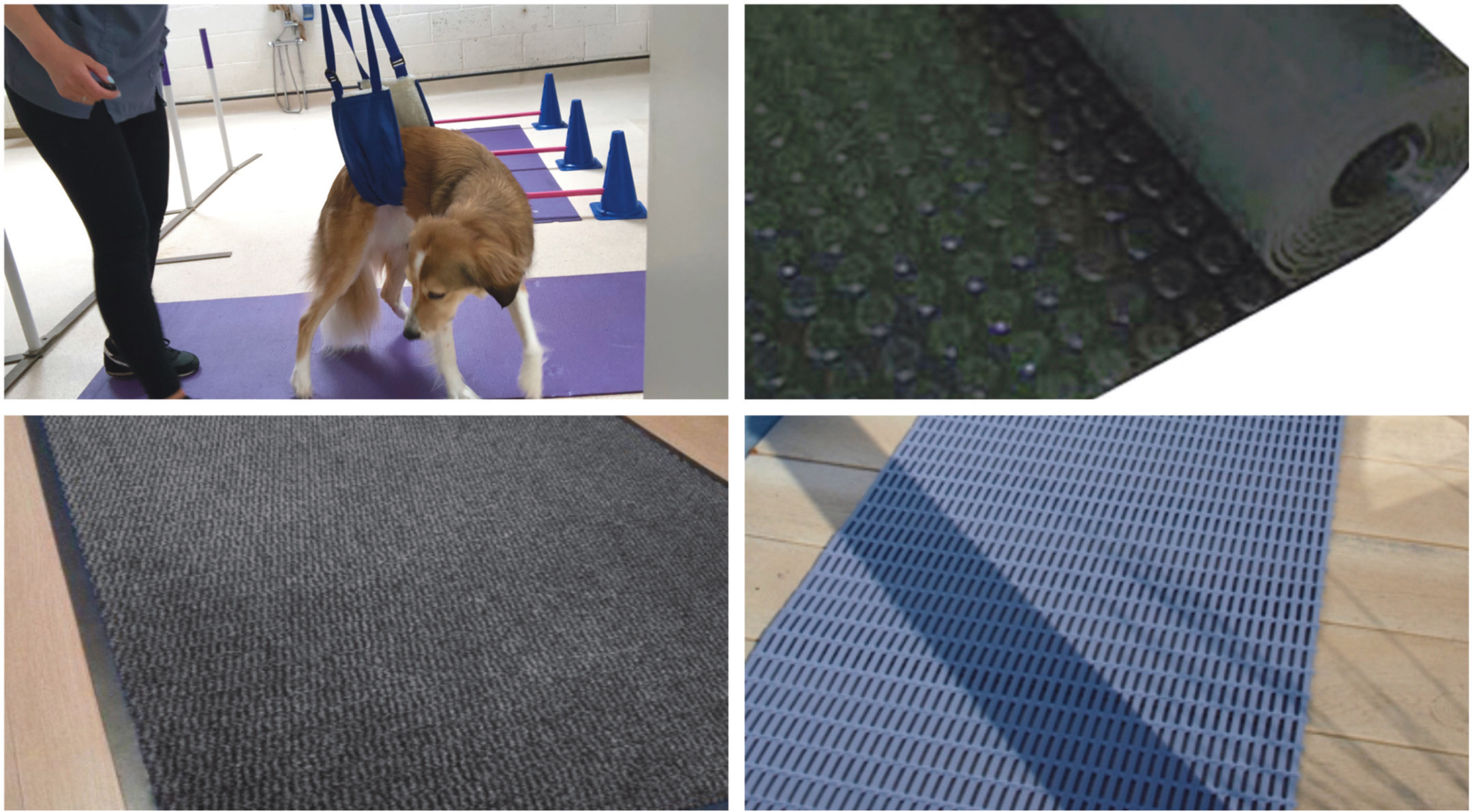
Use of a proprioceptive track, whereby the patient is walked over different textured surfaces which have been lined up such as carpet, rubber matting, bubble wrap and vet bedding further enhances proprioception (Dycus et al, 2017), and is also beneficial to include as part of the therapy session (Figure 6).
Surgical management
There are a number of surgical procedures which have been suggested to assist with the management of issues relating to the hip. The most common surgical procedures performed around the hip include femoral head and neck excision, used to treat Legg-Calvé-Perthes disease, femoral head fractures and manage some cases of hip dysplasia (Grisneaux et al, 2003), and total hip replacement. The goal following each of these surgeries is to rehabilitate the animal until they can achieve long-term pain-free use of the affected limb (Dycus et al, 2017).
Femoral head and neck excision
Femoral head and neck excision is used as a management tool for hip dysplasia, as it removes contact between the acetabulum and the femoral head, reducing pain secondary to joint disease and improving function (Harper, 2017). It is used as a treatment for Legg-Calvé-Perthes disease which is caused as a result of ischaemic necrosis to the femoral head, typically in young, small breed dogs (Cardoso et al, 2018).
Surgical removal of the femoral head and neck allows for the formation of a pseudoarthrosis made from dense fibrous tissue. Unlike the advice following many orthopaedic procedures, which is for the patient to rest in the immediate post-op period, following femoral head and neck excision early limb loading must be encouraged to prevent restrictive fibrous tissue forming which could severely limit the long-term available range at the coxofemoral joint (Harper, 2017). Passive range of motion exercises and controlled walking (starting with 5 minutes) should begin 48 hours after surgery, ensuring the patient is comfortable enough to facilitate this (Dycus et al, 2017). More active exercises are introduced at around 2 weeks postoperatively, and are selected on the basis that they promote hip extension or encourage limb loading and strengthening or core strengthening. Examples include:
- Hydrotherapy
- Weaving
- Walking over cavaletti poles
- Gentle incline walking
- Balance exercises as per those described above
A further 10-14 days after initiating these active exercises, the introduction of stairs and an increase in gait pace to include trotting can begin, as long as the dog is comfortable and progressing well.
There are long-term implications for animals having undergone femoral head and neck excision, as the affected limb is permanently shortened by the procedure, and as a result the dog will overextend the hock joint to compensate. Long term rehabilitation therapies may be required in some patients to help address these compensations.
It is useful to note that patient outcomes following femoral head and neck excision are considerably more favourable if there is good muscle mass present before the surgical procedure (Grisneaux et al, 2003). For this reason, if the procedure is elective, and the dog's pain levels can be managed, physiotherapy before surgery is advantageous. This may be more relevant when the procedure is performed for dogs with dysplasia, rather than those suffering from Legg-Calvé-Perthes disease, as those suffering with the latter are likely to be in a considerable amount of discomfort (Cardoso et al, 2018). It is also for this reason that early surgical intervention is preferable, where possible, as the chronicity of the condition is likely to attribute to further muscle atrophy, therefore increasing recovery time (Harasen, 2004).
Total hip replacement
In the immediate postoperative period (the acute phase, up to day 3) following total hip replacement, most dogs will remain hospitalised and the main focus is analgesia – primarily delivered in the form of pharmaceuticals, but which can be supplemented with rehabilitation techniques including electrotherapy and cryotherapy (Marcellin-Little et al, 2015). An abdominal sling should be used to facilitate early standing and to assist the dog with toileting, and its use should be continued at home until around 2-3 weeks post-surgery, at which point the dog can confidently use their limb (Marcellin-Little et al, 2015).
Avoidance of accidents to prevent implant luxation (which is the most common early complication) is paramount – so owner education on the use of non-slip flooring is key (Figure 6), as recovery rates in uncomplicated cases are excellent (Marcellin-Little et al, 2015).
In human patients, manual physiotherapy techniques are initiated early on in the recovery process in order to promote restoration of flexion and extension within the joint. In dogs, the same goals apply, and early intervention with range of motion techniques may assist with organisation of scar tissue, a reduction in pain and restoration of range of motion (Marcellin-Little et al, 2015). In the sub-acute phase of rehabilitation, this involves the inclusion of passive range of motion exercises, gentle stretching and early limb loading; avoiding exercises which would place unnecessary stress on the joint capsule and bone-implant interface. This generally means assisting the dog with walking in a straight line, avoiding adduction and abduction.
The chronic phase of rehabilitation involves strengthening the musculature of the limb which has undergone surgery and the other limbs (Marcellin-Little et al, 2015). For this, a very gradual introduction of the hind limb strengthening exercises described above for both conservatively managed dysplasia osteoarthritis and femoral head and neck excision would be beneficial to the patient. Studies suggest that normal body weight distribution to the operated limb is present at 3 months post-surgery (Lascelles et al, 2010).
Summary
Rehabilitation techniques play a vital role in the conservative management of chronic conditions affecting the hip, post-operatively and for the treatment of soft tissue injuries surrounding the hip joint. A good working relationship between the veterinary surgeon and the rehabilitation therapist is paramount to ensure the dog is comfortable and progressing well. As always, rehabilitation techniques should be performed by a qualified individual belonging to one of the following registers:
- Institute of Registered Veterinary and Animal Physiotherapists
- National Association of Veterinary Physiotherapists
- Register of Animal Musculoskeletal Practitioners
- Association of Chartered Physiotherapists in Animal Therapy.
KEY POINTS
- Issues affecting the hip are a common cause of lameness in the dog, especially among the young dog population.
- Important differential diagnoses include developmental conditions such as Legg-Calvé-Perthes disease and hip dysplasia, osteoarthritis of the hip, and soft tissue injuries, particularly if the dog has a history of participating in athletic activities.
- Soft tissue injuries to the hip area generally carry an excellent prognosis following rehabilitation, allowing a complete return to function for most dogs.
- The goals for rehabilitating the conservatively managed dysplastic hip and the arthritic hip are the same: improve joint range of motion (namely extension), strengthen musculature and help manage pain.
- Rehabilitating the patient following any surgical procedure to the hip focuses on early limb use, and in the case of femoral head and neck excision surgery it also focuses on promoting range of motion as soon as the patient is comfortable enough.