


Parasite distributions in UK cats and dogs continue to be very fluid, with changes in climate, habitat and movement of pets all playing a significant role. Changing conditions in the UK, alongside increases in pet travel and importation, make it difficult to predict where and when pathogens will emerge, and the risk they will pose to UK biosecurity, human and animal health.
Imported parasites
Increasing numbers of imported rescue cats and dogs have been seen over the past few years, with an associated risk of exotic pathogens entering the UK. The European Scientific Counsel for Companion Animal Parasites (ESCCAP) UK & Ireland does not support importation where pets can be rehomed in the country of origin. However, ESCCAP UK & Ireland is keen to work with charities to improve screening prior to importation and to raise awareness of the associated issues. ESCCAP UK & Ireland also supports charities working in countries around the world to improve animal welfare and reduce the need for animal relocation.
Echinococcus multilocularis, the cause of cystic echinococcosis, is a severe zoonosis. The adult tapeworm is carried by both foxes and domestic canids, with foxes acting as a reservoir of infection and microtine voles as intermediate hosts. Dogs and foxes become infected by predation of these voles, with infection in dogs bringing the parasite into close proximity to people. Cats can act as definitive hosts for E. multilocularis, but have a lower worm burden and fecundity than canids. E. multilocularis is widespread throughout Europe, but the UK currently remains free of the parasite due to compulsory tapeworm treatment of dogs with praziquantel prior to UK entry. However, the half-life of praziquantel is short, and so infection may occur in the 5-day window between compulsory treatment and entry into the UK. The illegal importation of pets also increases the risk of this parasites arrival. A survey of gastrointestinal parasites in dogs illegally entering the UK published this year found tapeworm in one of the 65 dogs examined (Fisher et al, 2023). Fortunately, it was not E. multilocularis, but could easily have been. This shows both the importance of the compulsory tapeworm treatment before entering the UK as well as treatment within 30 days after arrival.
Heartworm and Leishmania cases reported to ESCCAP UK & Ireland continue to remain high, and another case of leishmaniosis has been reported in an untravelled dog in the UK (McGrotty et al, 2023). The dog was living in a household with a Leishmania positive dog and horizontal transmission through close contact therefore seems very likely. Owners should be made aware of this possibility when rehoming Leishmania positive dogs. This is also a reminder that Leishmania infection needs to be considered as a differential diagnosis in dogs with relevant clinical signs living with other Leishmania positive pets, and in those whose parents have lived or travelled abroad. Clinical presentations are varied and commonly include lymphadenopathy, cutaneous signs (for example, generalised and focal alopecia, hyperkeratosis, dermal ulcers and periocular alopecia (Figure 1)), weight loss, splenomegaly, epistaxis and renal signs associated with glomerulonephritis. Polyarthritis, thrombocytopaenia, ocular inclusion bodies, uveitis and neurological signs associated with spinal and central nervous system granulomas may also be present.

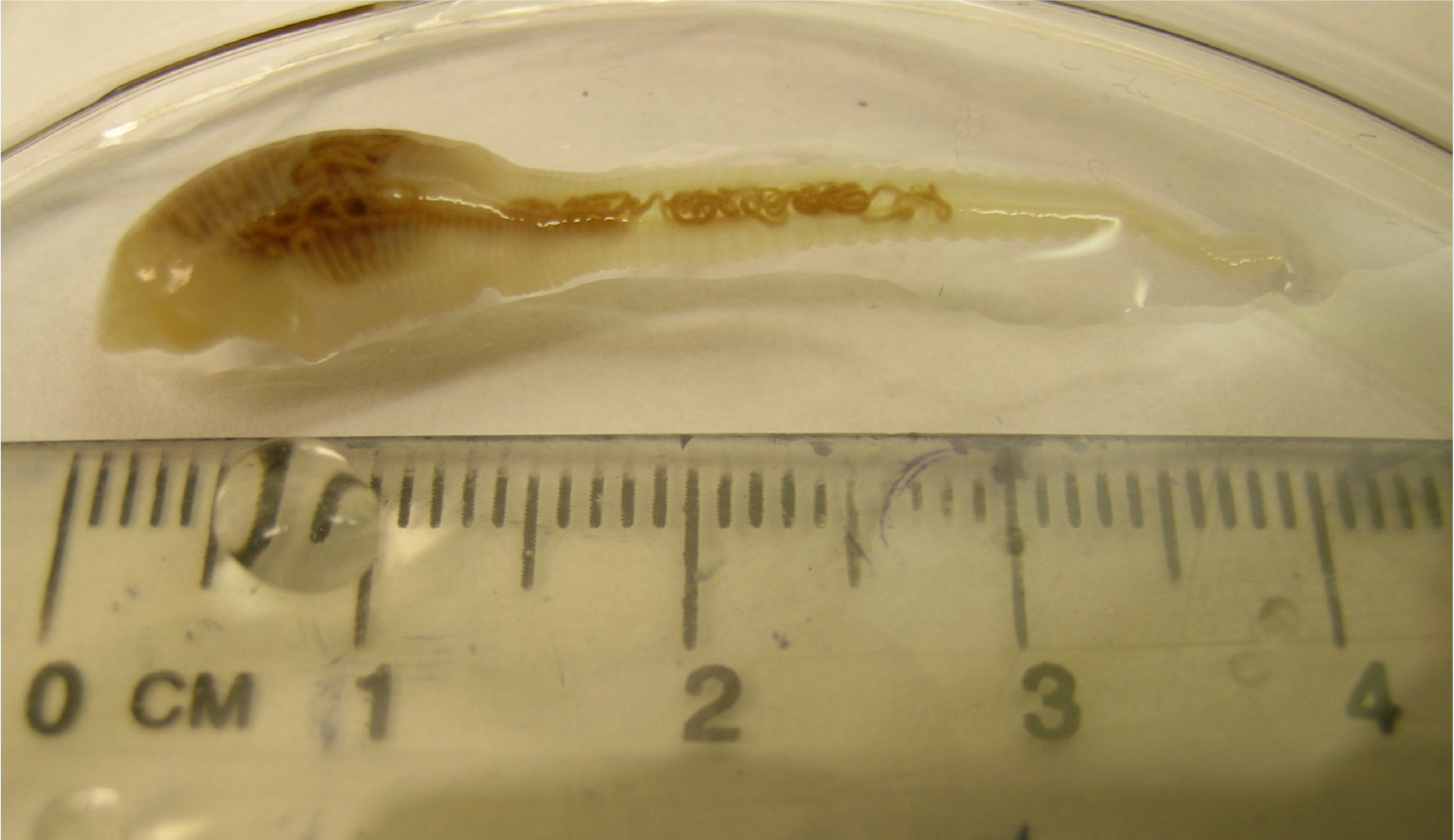
A number of imported dogs infected with the nasal pentastomid Linguatula serrata (‘tongue worm’) have been seen in the UK over the past 10 years from dogs imported from Romania and, more recently, Turkey (Mitchell et al, 2016 (Figure 2)). Infection is acquired from the consumption of raw meat and offal in endemic countries. L. serrata is a zoonotic infection with humans acting as intermediate as well as definitive hosts, and may therefore become infected through ingestion of eggs from nasal secretions and faeces. Most cases of infection in dogs are subclinical, however, large burdens can lead to rhinitis and nasopharyngitis with associated chronic sneezing and coughing, purulent nasal discharge and epistaxis. Recently, the first recorded case in an untravelled dog was reported in the UK (Campbell and Jones, 2023). The dog in question was on a raw diet and this is a possible source of infection. Adequate pre-freezing of raw food will kill the infective nymphs, but if not adequately pre-frozen, then infection via this route should be considered as a differential for dogs on raw diets.
Brucella canis is a Gram-negative coccobacilli bacteria predominantly infecting domestic dogs and many infections are clinically mild. Infection is typically associated with reproductive abnormalities, including infertility, abortion, endometritis, epididymitis and orchitis and scrotal oedema. A wide range of non-reproductive conditions can also occur, including chronic uveitis, endophthalmitis and discospondylitis. Lymphadenitis is common, along with non-specific clinical signs such as lethargy, exercise intolerance, decreased appetite and weight loss.
Transmission occurs via reproductive fluids, but the bacterium is also shed in urine, blood and saliva. Once dogs are infected, infection either persists for 2–3 years before elimination by the immune system, or lifelong infection is established. Antibiotic therapy is not effective at eliminating infection. B. canis is not currently endemic in the UK – but the risk of B. canis entering the UK in imported dogs has been highlighted (Middlemiss, 2021). This risk extends to veterinary professionals coming into contact with infected dogs in practice, as well as new owners and charity workers. B. canis is classed as a reportable disease under the Zoonoses Order and in 2022, the first full reporting year, 54 cases were reported. This is likely to be a significant underestimate of infection, given that clinical signs can be multi-fac-eted and vague and many cases are subclinical. Vigilance for relevant clinical signs in practice is vital, alongside screening dogs imported from endemic countries, both to reduce personal risk but also to help prevent establishment of this pathogen in the UK.
ESCCAP UK & Ireland continues to recommend that vets follow four key steps (the ‘four pillars’) when examining all imported dogs. These are:
- Checking for ticks and subsequent identification.
- Treating dogs with praziquantel within 30 days of their return to the UK in addition to the compulsory tapeworm treatment, and treating for ticks if a tick treatment is not in place.
- Recognising clinical signs relevant to diseases in the countries visited or country of origin.
- Screening for exotic parasites in imported dogs. For dogs imported into the UK, the following screening tests are recommended:
- Leishmania – quantitative serology and/or polymerase chain reaction.
- Heartworm – antigen blood test/Knott's test.
- Ehrlichia canis and Anaplasma spp – serology, polymerase chain reaction.
- Hepatozoon canis – blood smear and/or polymerase chain reaction.
- Babesia spp – polymerase chain reaction z Brucella canis – consult external lab for suitable test.
- Leishmania and heartworm testing should be repeated 6 months after importation and B. canis 3–6 months after importation.
A thorough clinical exam is also essential to identify relevant clinical signs and look for evidence of gross worm infestation, such as Thelazia callipaeda, Dirofilaria repens and Linguatula serrata. ESCCAP UK & Ireland has collaborated with the Animal and Plant Health Agency (APHA) to provide a free service for the identification and surveillance of these exotic parasites in UK dogs. This is vital to improve prognostic outcomes and to minimise the risk of exotic parasites becoming established in the UK. APHA will carry out free-of-charge, morphological identification of suspected cases of these parasites seen in veterinary practices in England and Wales. Samples submissions should be posted to the APHA Carmarthen Veterinary Investigation Centre, and must be accompanied by full clinical history to qualify for free testing.
Lungworm
Relatively mild weather in 2021 and into 2022 has likely supported continuing slug activity and numbers. ESCCAP UK & Ireland has also seen an increase in reported case queries of angiostrongylosis in 2023. This includes a case from a practice in Inverness, demonstrating that it is present in endemic foci from its traditional heartlands in the south of England and Wales right up to the far north of Scotland. Veterinary professionals should therefore continue to be vigilant for cases of Angiostrongylus vasorum in their area and advise preventative treatment for high-risk dogs (previously infected dogs, dogs living in close proximity to other cases, those that are coprophagic, eat slugs, snails, grass and/or amphibians). As well as preventative treatment for dogs whose geographical location and lifestyle puts them at risk of exposure from A. vasorum, simple precautions, such as bringing in toys, food and water bowls indoors at night and avoiding walking after periods of rain, will also help to minimise any risk of transmission by this route.
Ticks
SAVSNET real-time tick data has shown another lengthy peak of activity from early spring to late autumn in 2022 as well as continued activity throughout December. It is important that pet owners remain aware of the possibility of exposure for both themselves and their pets at any time of year, especially from early spring through to late autumn. This supports previous real-time data demonstrating this trend (Wright et al, 2018).
A range of tick-borne pathogens are present in the UK and/or in travelled dogs. A recent study looked at 76 dogs diagnosed with tick-borne diseases in the UK between 2005 and 2019 (Silvestrini et al, 2023). In total, 25 were diagnosed with ehrlichiosis, 23 with babesiosis, eight with Lyme borreliosis and six with anaplasmosis. In total, 14 dogs had co-infections with two or three pathogens. Except for those dogs with anaplasmosis and Lyme borreliosis, most dogs with tick-borne diseases had a history of travel to or from endemic countries. However, three dogs with ehrlichiosis, and one dog each infected with Babesia canis and Babesia vulpes did not have any history of travel. B. vulpes is thought to be endemic in the UK, likely carried by foxes. Foci of Dermacentor reticulatus ticks capable of transmitting B. canis has long been established in Britain in West Wales, Devon, Essex and London (Medlock et al, 2017), presenting an opportunity for B. canis to establish endemic foci if introduced via infected dogs or ticks. This occurred in the winter of 2014/2015 when an endemic focus of B. canis infection was established in Harlow, Essex. The parasite was confirmed both in local Dermacentor ticks and untravelled dogs (Phipps et al, 2016). Recent studies have failed to find the parasite persisting in these foci, but found another infected tick in Devon, demonstrating the potential for further endemic foci to occur (Sands et al, 2022).
Tick-borne encephalitis virus may infect a variety of mammalian hosts including dogs, foxes and ruminants. It is a potentially severe zoonosis, with infections most commonly resulting in a transient fever, but sometimes progressing to menigioencephalititis, central nervous system signs and death. The European virus has spread rapidly and is endemic in Scandinavia, western, central and eastern Europe. UK surveillance has found strong evidence that it is present in both the New and Thetford Forests in the UK (Holding et al, 2020). A case in an untravelled member of the public in Yorkshire this year suggests that the virus may have spread to new areas of England. The risk from this pathogen to humans and dogs needs to be kept in perspective, but for people and dogs at high risk of tick exposure it is another good reason to have tick prevention in place before enjoying the great outdoors.
Preventative strategies include:
- Preventative tick treatments – the use of licensed preventative products that rapidly kill or repel ticks are useful in reducing tick feeding and therefore transmission of infection. Products containing an isoxazoline or pyrethroid fulfil these criteria. No product is 100% effective and owners should therefore still be advised to check their pet for ticks at least every 24 hours if possible.
- Checking for ticks at least every 24 hours – latest tick surveillance scheme data suggests that the majority of ticks are located and found around the head, face, legs and ventrum (Wright et al, 2018). Nymphs are extremely small and easily missed, so tick removal alone should not be relied upon for high-risk cats and dogs. Ticks should be removed with a tick removal device. After ticks have been removed, they can be submitted to the tick surveillance scheme for identification.
- Sticking to paths, where possible, will greatly reduce the risk of tick exposure.
What is the rest of 2023 likely to hold?
Risk assessment is likely to be a major focus for the rest of 2023 and 2024 as hopefully more domestic data become available for a range of parasites. Ongoing vigilance for exotic parasites in imported pets will also remain important as an increasing range of exotic parasites continue to be identified in UK dogs. B. canis remains a concern, both in terms of zoonotic risk to pet owners and also to the wider public and veterinary professionals. Whether legislation will be brought in to make testing compulsory for this pathogen before entry into the UK remains to be seen.
Resources
- There is new CPD available discussing these parasites and the free service APHA and ESCCAP UK & Ireland provides on the Vet Times website: https://cpd.vettimes.co.uk/cpd-plus/companion-animal/cpd-parasitology/exotic-worms-and-worm-like-parasites-and-surveillance-in-the-uk and on YouTube: https://www.youtube.com/watch?v=8n1RS2u_c4s
- Posters are available on the ESCCAP UK & Ireland website to help identify exotic parasites and ticks associated with imported dogs: https://www.esccapuk.org.uk/parasite-id-posters-uk/
- Bristol University has an excellent tick identification website: http://www.bristoluniversitytickid.uk/